Taking inspiration from a marketed treatment for Duchenne muscular dystrophy (DMD), this post explores the possibility of defining and measuring the marginality of a therapy for a degenerative disease.
The DEDUCTION Project is the latest—and possibly conclusive—development within the DTAT research programme. This post explains its origins, motivation and current outlook.
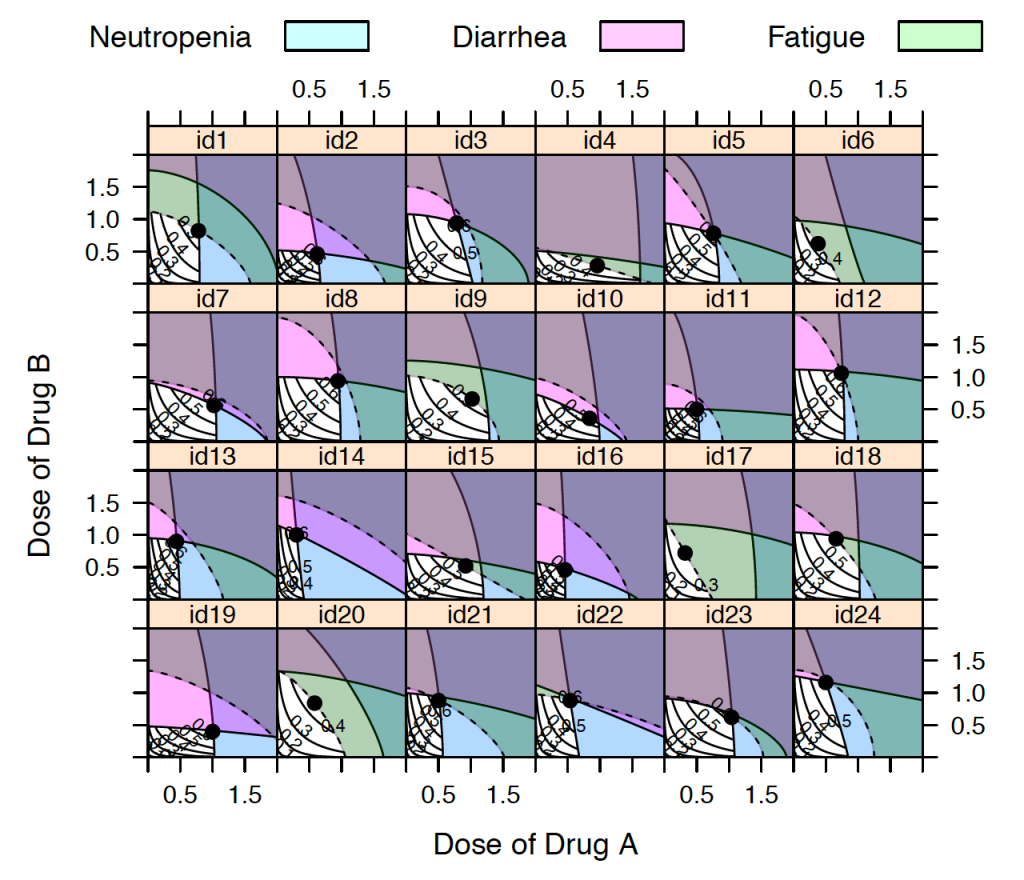
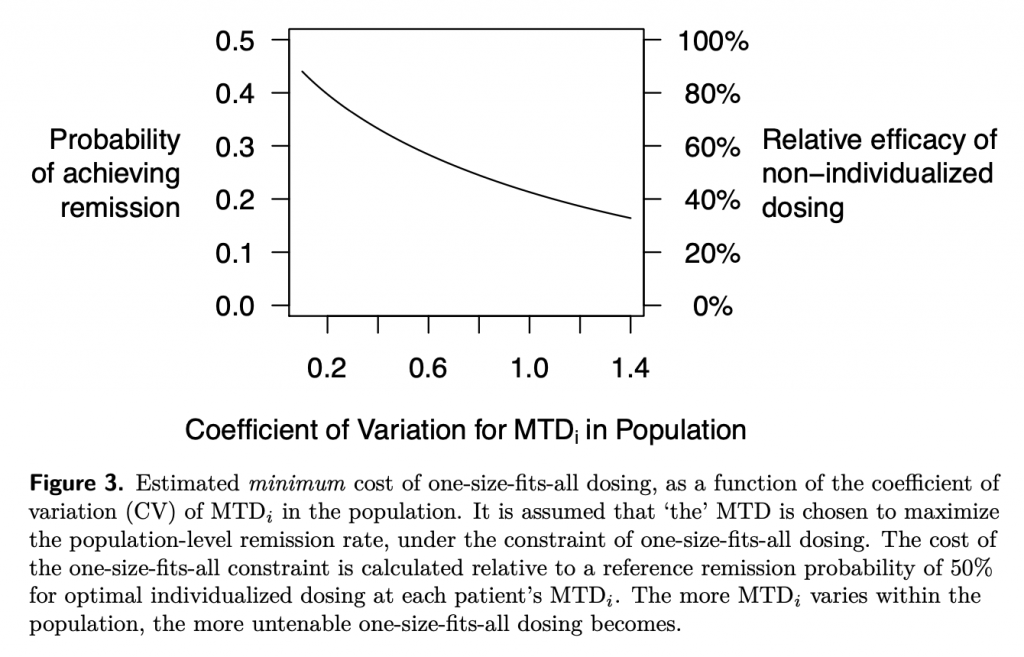
This is a lay explanation for my paper accepted for publication in a CPT: Pharmacometrics & Systems Pharmacology special themed issue on Dose Optimization in Oncology
precautionary